
By R. Yespas. Johnson and Wales University.
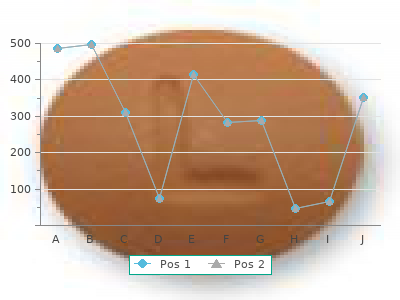
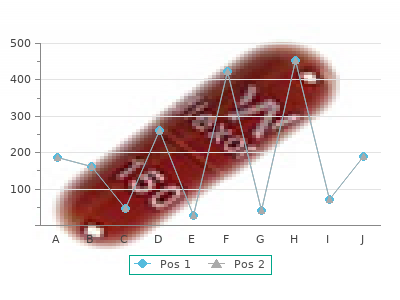
At the time it was written it was central to the contemporary emphasis on a need to acknowledge how uninformed patients were discount 500mg meldonium with visa. This paper examines the different models of health professional’s behaviour and emphasizes the role of health professional’s health beliefs buy 500 mg meldonium with amex. This theoretical paper examines the background to the recent interest in compliance and discusses the relationship between compliance and physician control meldonium 250 mg amex. It set the scene for much subsequent research and shifted the emphasis from doctor as expert to seeing the consultation as an interaction. The history of theories of addictive behaviours and the shift from a disease model of addictions to the social learning theory perspective is then described. The chapter also examines the four stages of substance use from initiation and maintenance to cessation and relapse, and discusses these stages in the context of the different models of addictive behaviours. The chapter concludes with an examination of a cross-behavioural perspective on addictive behaviours and an assessment of the similarities and differences between smoking and drinking and their relationship to other behaviours. This chapter covers: ➧ The prevalence of smoking and alcohol consumption ➧ What is an addiction? This decrease in smoking behaviour follows a trend for an overall decline and is shown in Figure 5. However, the data also showed that, although women smoke fewer cigarettes than men, fewer women than men are giving up. Smokers can also be categorized in terms of whether they are ‘ex-smokers’, ‘current smokers’ or whether they have ‘never smoked’. The trends in smoking behaviour according to these categories are shown in Figure 5. Again, sex differences can be seen for these types of smoking behaviour with men showing an increase in the numbers of ‘never smoked’ and ‘ex-smokers’, and a decrease in ‘current smokers’, whilst women show the same profile of change for both ‘current smokers’ and ‘ex-smokers’ but show a consistently high level of individuals who have ‘never smoked’. In general, data about smoking behaviour (General Household Survey 1994) suggests the following about smokers: s Smoking behaviour is on the decline, but this decrease is greater in men than in women. About 27 per cent of men and 11 per cent of women were drinking more than the recommended sensible amounts of alcohol which at this time were 21 units for men and 14 units for women. Negative effects Doll and Hill (1954) reported that smoking cigarettes was related to lung cancer. Since then, smoking has also been implicated in coronary heart disease and a multitude of other cancers such as throat, stomach and bowel. In addition, the increase in life expectancy over the past 150 years is considerably less for smokers than for non-smokers (see Chapter 2). In industrialized countries smoking is the leading cause of loss of healthy life years. The average smoker dies eight years early and starts to suffer disability 12 years early whilst a quarter of smokers who fail to stop die an average of 23 years early (West and Shiffman 2004). It has been suggested that smokers report positive mood effects from smoking and that smoking can help individuals to cope with difficult circumstances (Graham 1987). For example, alcoholism increases the chance of disorders such as liver cirrhosis, cancers (e. In a longitudinal study, Friedman and Kimball (1986) reported that light and moderate drinkers had lower morbidity and mortality rates than both non-drinkers and heavy drinkers. They argued that alcohol consumption reduces coronary heart disease via the following mechanisms: (1) a reduction in the production of catecholamines when stressed; (2) the protection of blood vessels from cholesterol; (3) a reduction in blood pressure; (4) self-therapy; and (5) a short-term coping strategy. The results from the General Household Survey (1992) also showed some benefits of alcohol consumption with the reported prevalence of ill- health being higher among non-drinkers than among drinkers. However, it has been suggested that the apparent positive effects of alcohol on health may be an artefact of poor health in the non-drinkers who have stopped drinking due to health problems. In an attempt to understand why people smoke and drink, much health psychology research has drawn upon the social cognition models described in Chapter 2. However, there is a vast addiction literature which has also been applied to smoking and drinking. Many theories have been developed to explain addictions and addictive behaviours, including moral models, which regard an addiction as the result of weakness and a lack of moral fibre; biomedical models, which see an addiction as a disease; and social learning theories, which regard addictive behaviours as behaviours that are learned according to the rules of learning theory. The multitude of terms that exist and are used with respect to behaviours such as smoking and alcohol are indicative of these different theoretical perspectives and in addition illustrate the tautological nature of the definitions. For example: s An addict: someone who ‘has no control over their behaviour’, ‘lacks moral fibre’, ‘uses a maladaptive coping mechanism’, ‘has an addictive behaviour’. These different definitions indicate the relationship between terminology and theory. For example, concepts of ‘control’, ‘withdrawal’, ‘tolerance’ are indicative of a biomedical view of addictions. Concepts such as ‘lacking moral fibre’ suggest a moral model of addictions, and ‘maladaptive coping mechanism’ suggests a social learning perspective. In addition, the terms illustrate how difficult it is to define one term without using another with the risk that the definitions become tautologies. Questions about the causes of an addiction can be answered according to the different theoretical perspectives that have been developed over the past 300 years to explain and predict addictions, including the moral model, the 1st disease concept, the 2nd disease concept and the social learning theory. These different theories and how they relate to attitudes to different substances will now be examined. However, parallels can be seen between changes in theoretical perspective over the past 300 years and contemporary attitudes. The seventeenth century and the moral model of addictions During the seventeenth century, alcohol was generally held in high esteem by society. It was regarded as safer than water, nutritious and the innkeeper was valued as a central figure in the community. In addition, at this time humans were considered to be separate from Nature, in terms of possessing a soul and a will and being responsible for their own behaviour. Animals’ behaviour was seen as resulting from biological drives, whereas the behaviour of humans was seen to be a result of their own free choice.

Critical illness and sedation can mask many of these symptoms buy meldonium 250mg on-line, but not the discomfort problems for patients order meldonium 250 mg visa. Removing intravascular fluid encourages replacement by extravascular fluid discount meldonium 500 mg on line, but limited transfer occurs during the few hours of haemodialysis, whereas continuous treatments (e. It mimics human glomerular filtration, as plasma is forced under pressure through a semipermeable Haemofiltration 347 membrane (ultrafiltration), and solutes are drawn across the membrane by convection. Unlike the human kidney, haemofiltration (and haemodialysis) cannot selectively reabsorb. Ultrafiltrate volumes are large (although smaller than healthy human ultrafiltrate), so that large infusions are needed to mimic reabsorption. Driving pressure was therefore the differential between a patient’s arterial and venous blood pressures. Anticoagulation was added to prevent thrombus formation in extracorporeal circuits; replacement fluid was given to mimic tubular reabsorption. Manufacturers are rationalising terminology by renaming ‘arterial’ circuits ‘afferent’ and ‘venous’ circuits ‘efferent’; this follows human renal physiology, and is logical, and so although not (as yet) universal, it is used here. Compared with haemodialysis, haemofiltration: ■ enables filtration despite hypotension ■ improves cardiovascular stability ■ enables more gentle removal of solutes (less disequilibrium) ■ removes significantly larger fluid volumes High-speed haemofiltration for short periods may achieve better clearance than haemodialysis, but circuits are relatively costly and time-consuming to prime, and the use of intermittent filtration is almost exclusively confined to hospitals with on-site renal units (Amoroso et al. Haemodiafiltration Ultrafiltrate countercurrent was not used with early haemofilters, so solute clearance remained poor once ultrafiltrate concentrations in filters approached plasma levels. Most units now add countercurrent to haemofiltration, calling it simply ‘haemofiltration’ (literature describing haemofiltration may not always clarify whether it refers to systems with or without countercurrents). Intensive care nursing 348 Theoretically, countercurrent clearance is proportional to countercurrent volume, but exchanges above 2–3 litres per hour do not significantly increase clearance (Miller et al. Prediluting blood (before the filter) reduces viscosity, increasing filtrate volume, urea clearance and filter life (reducing need for anticoagulation) (Kaplan 1985a); but anecdotal reports suggest predilution both hastens coagulation and reduces filter life, perhaps due to activation of clotting factors; further research is needed both to identify mechanisms and to guide practice. Free-flow ultrafiltrate relies on gravity (height difference between the filter and collection bag) to create negative pressure, but most systems now control ultrafiltrate with volumetric pumps, so that the ultrafiltrate pump speed determines negative pressure. Filter membranes Cuprophane or cellulose, used for early filters (Kwan 1997), activate the immune complement system, releasing highly vasoactive substances (e. These cause: ■ hypotensive crises ■ neutropenia Haemofiltration 349 ■ thrombocytopenia ■ hypoxia (neutrophil sequestration in pulmonary circulation). Often containing more than 20,000 fine capillary 2 tubes, they have large surface areas (often 2 m (Ervine & Milroy 1997)), a small volume and, being cylindrical, they are also sturdy. Small capillary tube diameter (65 micrometres (Ervine & Milroy 1997)) usually necessitates anticoagulation to prevent thrombosis and obstruction. Ervine and Milroy (1997) suggest hollow fibre threshold is usually about 30 kDa, but various pore-size filters are available: most of the filters now used can double this threshold. Fibres are glued with polyurethane, making them less biocompatible than flat plate filters (Molnar & Shearer 1998). Although overall surface area is smaller than with hollow fibres, flat plates can clear small molecules more efficiently (Hinds & Watson 1996) and are less prone to clotting, and so require less anticoagulation. Most systems now measure transmembrane pressure directly, although some older systems may still rely on indirect indications (e. Transmembrane pressure is created by various factors, but rising pressure usually suggests significantly decreased filtration surface area from thrombus formation (efferent filters protect patients from emboli). While priming removes air emboli, its main purpose is the removal of glycerol and ethylene oxide used to protect filters during storage and transportation. These chemicals can cause convulsions, paralysis, renal failure and haemolysis (Martindale 1996), so that priming volumes should follow manufacturers’ recommendations and not be abandoned once circuits are filled with fluid. As with human nephrons, solute clearance is limited by ultrafiltrate concentrations, ending once equilibrium is reached. Pore sizes of human nephrons and artificial filters are normally large enough to clear anything potentially in blood apart from blood cells. Early filters allowed solutes of 30 kDa to pass—many are now more porous—but actual clearance varies with: ■ molecular size ■ It ultrafiltrate concentration ■ protein binding. Intensive care nursing 350 The use of lactate-based dialysate fluids can accentuate problems with acidosis; bicarbonate filtration (Hilton et al. Patients who are being haemofiltered are often ventilated, unconscious, monitored and receiving many drugs (often including large dose inotropes); their dependent state necessitates fundamental aspects of care (comfort, hygiene, pressure care), while family and friends of critically ill patients are often anxious, needing more time spent with them. Care may have to be prioritised to maintain safety; such workloads illustrate the dangers of assuming that one-to-one nurse-patient ratios are always safe. Large filtrate and replacement volumes, together with many other inputs and outputs, can make calculations complex, increasing risks of fluid balance calculation error. The risk of fluid balance error can be reduced by rationalising fluid balance charts. Insensible loss in health is about 500 ml each day, rising to a litre or more with critical illness: fluid balance charts are necessarily inaccurate by 500–1,000 ml. Measuring decimal points of millilitres achieves little beyond pedantry and possible carelessness with larger figures (centilitres and litres); fluid balance charts and calculations are safer if rationalised. Calculators can assist complex calculations, but major errors can occur by accidentally catching keys, and so larger figures (e. Extracorporeal circuits are (usually) continuously anticoagulated to prevent thrombus (and embolus) formation. Although efferent filters should remove emboli before reaching patients, adsorption of blood proteins onto foreign surfaces (e. The signs of thrombus formation include: ■ dark blood in circuits ■ kicking of lines ■ high transmembrane pressure ■ reduced filtration (if not pump-controlled). Anticoagulation may be unnecessary with prolonged clotting times or when afferent flow exceeds 300 ml/min (McClelland 1993a). Heparin prime reduces initial platelet aggregation, enabling a lower dose of subsequent anticoagulants. Anticoagulants are Haemofiltration 351 below filter threshold, but some inevitably reach patients, aggravating coagulopathies; reversal agents (e.
Nurses work with families and with individ- design a system for delivery of nursing care ual family members buy discount meldonium 250 mg line. The of nursing research and education in a large mu- family is also viewed as an interpersonal system cheap 500 mg meldonium fast delivery. Congruence in ment used my framework and Theory of Goal perceptions of nurse and family members helps in Attainment (Benedict & Frey buy 250 mg meldonium with visa, 1995). The Theory of assessing a situation to identify concerns and/or Goal Attainment was used in adult orthopedic problems in the interpersonal system. Two cases were presented and the use Sneed (1991) stated that my interactive systems ap- of the Theory of Goal Attainment was described in proach of goal attainment is an ideal basis for each situation. This group used Community Health my theory with inpatient juvenile sexual offenders, offenders in maximum security, and community Community health nursing involves a variety of parolees. For example, school nurses must understand the edu- Continuous Quality Improvement cation system. Occupational health nurses must Continuous quality improvement in nursing and understand the political system, the economic sys- health care is a reality. Structure provides an overall organi- health programs as they interact and set goals with zation of the program. Process relates to nursing interdisciplinary teams to manage health care activities. Outcomes are separate from but related (Hampton, 1994; Sowell & Fuszard, 1989; Sowell & to performance criteria for evaluation of nursing Lowenstein, 1994). In this sense, they system provides structure for a continuous quality- are relating to the interpersonal systems in the improvement program (King, 1994). This is done within a variety of social action Process Model in my Theory of Goal systems in the community. Although the focus is Attainment gives a process that leads to goal attain- groups, nurses work with individuals for whom ment that represents outcomes. An example was given to 16–1) shows the interactions of the three systems in document effectiveness of nursing care if one uses community health. The record system is an information system based on Use in Hospitals my Theory of Goal Attainment. The record system Two case studies were presented to demonstrate can be designed and adapted to most health-care nurses’ use of the transaction process and knowl- systems. For nurses, it was designed to gather data edge of the concepts of perception, communica- from assessments of the patient, make a nursing tion, interaction, and role (King, 1986b). King’s Theory of Goal Attainment 243 nursing care, and write mutually agreed-upon goals twentieth century to the science of nursing in the and means to attain them. Elements in the goal-oriented nursing record are: (1) data base, (2) goal list, (3) nursing orders, (4) flow sheets, (5) progress notes, and (6) discharge summary. My conceptual Several nurses have tested the theory in research on system and transaction process in the Theory aging, parenting, psychiatric-mental health, and of Goal Attainment provides one approach to ambulatory care (Alligood et al. For interaction between nurses and health- ducted studies in their cultures to test the Theory of care professionals and between health- Goal Attainment (Coker et al. For common discourse among health pro- and responses to professional nursing care that fessionals and between nurses and nursing resulted in an instrument that measures patient personnel. Direct measure of outcomes resulting in My vision for the future of nursing is that nursing quality care and cost-effective care; that is, will provide access to health care for all citizens. One valid and reliable assessment instru- are directed to the right place in the system for ment to assess activities of daily living as a nursing care, medical care, social services informa- basis for goal-setting. For continuity of care within and between tion process will be used by every practicing nurse health-care agencies. Theory of Goal Attainment, and Transaction Process Model will continue to serve a useful pur- When knowledge of the concepts and the pose in delivering professional nursing care. The transaction process has been used in hospi- ideas have been tested in research and in practice, tals, homes, nursing homes, and community and nurses in education and practice have used the health agencies, nurses have been motivated knowledge of the concepts. The relevance of to seek additional knowledge in formal edu- evidence theory–based practice, using my theory, cational programs. Publications, including Frey & Sieloff (1995), identified from a review of the literature, will be summarized and briefly discussed. Finally, of King’s recommendations will be made for future knowl- edge development in relation to King’s Interacting Systems Framework and midrange theory, par- Theory of Goal ticularly in relation to the importance of their application within an evidence-based practice environment. Attainment Christina Leibold Sieloff, Maureen Application of Interacting Frey, & Mary Killeen Systems Framework In conducting the literature review, the authors began with the broadest category of application— application within the Interacting Systems Frame- Application of Interacting Systems work to nursing care situations. Because a con- Framework In conducting the literature review, the Concept Development Within the authors began with the broadest category Framework of application—application within the Interacting Systems Framework to nursing Theory of Goal Attainment care situations. Recommendations for Knowledge Development Related to King’s ceptual framework is, by nature, very broad and Framework and Theory abstract, it can only serve to guide, rather than prescriptively direct, nursing practice. Summary King’s Interacting Systems Framework has been used to guide nursing practice in several References ways. Fawcett, Vaillancourt, and Watson (1995) used the frame- Since the first publication of Dr. Imogene King’s work to guide nursing practice in a large tertiary work (1971), nursing’s interest in the application of care hospital. The fact that she the framework to guide nursing practice with spe- was one of the few theorists who generated both a cific patient populations. Doornbos (2002) ex- framework and a midrange theory further ex- plored family health in families with chronically panded her work. Table 16–1 delineates other appli- to publish and examine new applications of her cations related to King’s Interacting Systems work. Alligood (1995) applied the theory to within the Framework orthopedic nursing with adults.
When drugs are prescribed to children that are Clinical Pharmacology 2003; 56: 489–93 buy 500 mg meldonium amex. Prescribers take sole responsibility for prescribing disposition generic 250 mg meldonium visa, action and therapy in infants and children best 250mg meldonium. The elderly are subject to a variety of complaints, many of which are Absorption of carbohydrates and of several nutrients, includ- chronic and incapacitating, and so they receive a great deal of ing iron, calcium and thiamine, is reduced in elderly people. There is a growing evidence base for the use of Lipid-soluble drugs are absorbed by simple diffusion down drugs in elderly patients, with important implications for pre- the concentration gradient (Chapter 3), and this is not scribing of many important classes of drugs, including statins, impaired by age. However, age per se does not affect drug angiotensin receptor blockers, vitamin D and bisphosphonates absorption to a large extent (Figure 11. Adverse drug reactions and drug interactions become more common with Drug increasing age. In one survey in general ↓Intestinal blood flow practice, 87% of patients over 75 years of age were on regular drug therapy, with 34% taking three to four Absorption↔ different drugs daily. The most commonly prescribed drugs were diuretics (34% of patients), analgesics (27%), ↓Weight tranquillizers and antidepressants (24%), hypnotics (22%) ↓Lean body mass and digoxin (20%). All of these are associated with a high ↑Fat ↓Hepatic blood flow incidence of important adverse effects. Drug elimination becomes less efficient with increasing ↓Concentration of age, leading to drug accumulation during chronic dosing. Homeostatic mechanisms become less effective with water-soluble drugs advancing age, so individuals are less able to compensate for adverse effects, such as unsteadiness or postural Metabolism↓ hypotension. The central nervous system becomes more sensitive to the actions of sedative drugs. Increasing age produces changes in the immune response ↓Renal blood flow Excretion↓ that can cause an increased liability to allergic reactions. Impaired cognition combined with relatively complex dose regimens may lead to inadvertent overdose. Although diazepam and lidocaine, whereas the distribution of polar glomerular filtration rate declines with age, this is not necessar- drugs such as digoxin is reduced compared to younger adults. The reduced clearance of benzodiazepines and to estimate this if necessary using a nomogram (see has important clinical consequences, as does the long half-life of Chapter 7) that incorporates height and weight, as well as age, several active metabolites (Chapter 18). Consequently, confusion or memory the elderly secondary to reduced renal excretion and/or impairment may be falsely attributed to ageing rather than to hepatic clearance are listed in Table 11. The principal age-related changes in pharmacokinetics are summarized in Figure 11. Key points 120 Key points 100 Pharmacokinetic changes in the elderly include: 80 • Absorption of iron, calcium and thiamine is reduced. It is Atenolol common clinical experience that benzodiazepines given to the Cimetidine elderly at hypnotic doses used for the young can produce pro- Diazepam longed daytime confusion even after single doses. The inci- Digoxin dence of confusion associated with cimetidine is increased in Non-steroidal anti-inflammatory drugs the elderly. Other drugs may expose physiological defects that Oral hypoglycaemic agents are a normal concomitant of ageing. Key points The prescription of hypnotics (see Chapter 18) should be Pharmacodynamic changes in the elderly include: minimized and restricted to short-term use. Although depression is common in old age and may indeed phenothiazines, beta-blockers, tricyclic antidepressants, need drug treatment, this is not without risk. Tricyclic antide- pressants can produce worthwhile remissions of depression but should be started at very low dosage. They are generally well This is commonly due to a failure of memory or to not under- tolerated by the elderly, although hyponatraemia has been standing how the drug should be taken. It is therefore essential that the drug regimen is kept as simple as possible The anticholinergic group of anti-parkinsonian drugs (e. There is scope for improved methods trihexyphenidyl, orphenadrine) commonly cause side effects of packaging to reduce over- or under-dosage. Glaucoma regimens are confusing and increase the risk of adverse inter- may be precipitated or aggravated and confusion may occur actions (see Chapter 13). Cerebral function in old people is easily disturbed, resulting in disorientation and confusion. It is shorter time, their sleep is more likely to be broken and they are important to start with a low dose and monitor carefully. Before hypnotics are commenced, other possible factors likely to suffer severe consequences, such as falls/fractures should be considered and treated if possible. Hypokalaemia due to decreased potassium intake (potassium-rich foods are often expensive), faulty homeo- Diabetes is common in the elderly and many patients are static mechanisms resulting in increased renal loss and the con- treated with oral hypoglycaemic drugs (see Chapter 37). It is comitant use of diuretics is more common in the elderly, and is best for elderly patients to be managed with diet if at all possi- a contributory factor in some patients. In obese elderly diabetics who remain symptomatic on prescribed when there is no indication for it (e. In one drugs because of the risk of hypoglycaemia: chlorpropamide series of geriatric patients on digoxin, the drug was withdrawn (half-life 36 hours) can cause prolonged hypoglycaemia and is in 78% of cases without detrimental effects. Brisk diuresis in patients with mental impairment or reduced The decline in renal function must be borne in mind when an mobility can result in incontinence. For many patients, a thia- antibiotic that is renally excreted is prescribed, especially if it is zide diuretic, such as bendroflumethiazide, is adequate. Appendix 3 diuretics, such as furosemide, should be used in acute heart of the British National Formulary is an invaluable practical guide.
8 of 10 - Review by R. Yespas
Votes: 336 votes
Total customer reviews: 336